
*DISCLAIMER: Selective Androgen Receptor Modulators (SARMs) are not approved by the FDA for any currently acceptable medicinal/therapeutic purpose. Therefore, this article does not serve as medical advice and is not to be intended to be used to diagnose, treat, cure or prevent any disease. SARMS are to be used for research purposes only and not intended for human consumption.*
What is LGD-3303?
LGD-3303 (not to be confused with LGD-4033, otherwise known as Ligandrol) is a relatively lesser-known compound compared to other SARMs out there. It was synthesized primarily for the treatment of osteoporosis and manufactured by Ligand Pharmaceuticals™; the same company responsible for the development of LGD-4033 (Ligandrol) and GW-501516 (Cardarine).
LGD-3303 is a nonsteroidal, orally-administered androgen receptor (AR) agonist that binds to the AR with high affinity. It has been reported to have great potency specific to skeletal muscle tissue, while simultaneously possessing substantially reduced levels of activity on the prostate [1].
Animal Data
Selectivity for Skeletal Muscle
In order to understand how LGD-3303 selectively exerts its effects on muscle tissue, we first must take a look at how researchers commonly examine this phenomenon in research.
The levator ani muscle, a group of 3 muscles located within the pelvis, is often used as a measure of anabolic activity in preclinical research involving anabolic/androgenic compounds. Below is an illustration of its anatomy in humans:
![]()
An effective way in which to test the effectiveness of anabolic agents in animals is to test them within the context of a castration model, where the animal’s testicles are removed. This inhibits the body’s ability to produce androgens, ultimately resulting in the muscle and prostate drastically reducing their original size and mass.
A 2009 study revealed that LGD-3303 was able to negate the negative effects that castration had on rats using a dose of 1mg/kg/day. This was illustrated by a significant increase in the rats’ levator ani to a similar level to that of the non-treated castrated group (otherwise known as a “sham” in scientific literature) [2]. In addition to this, the muscle weight of the castrated rats treated with LGD-3303 surpassed the muscle weight of what would be considered typically achievable by a normal, non-castrated rat.
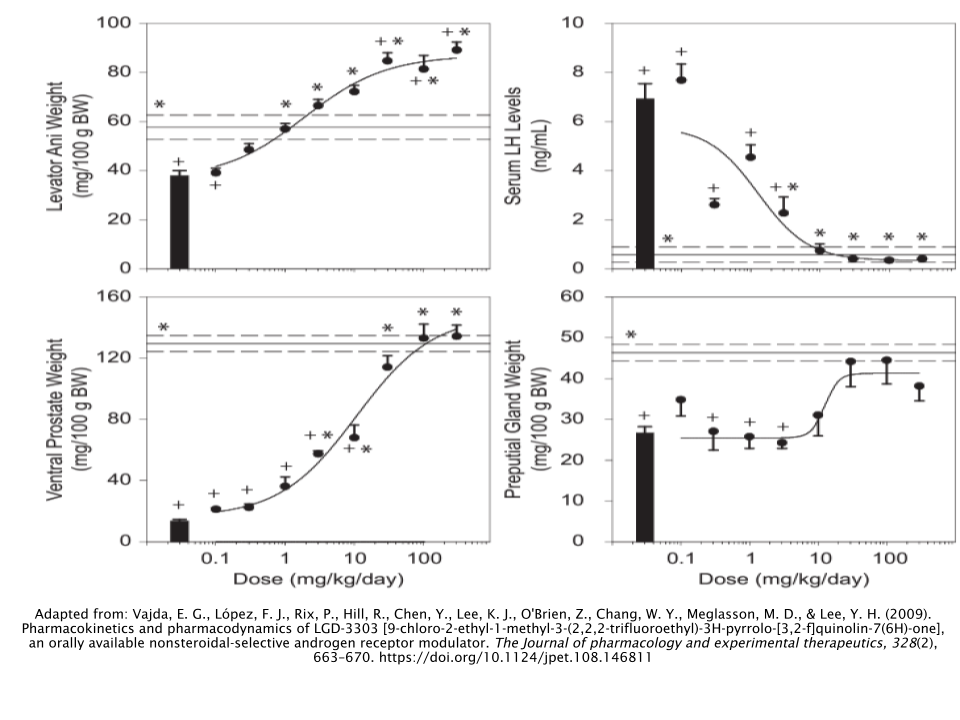
As illustrated in the figure above, LGD-3303 was able to elicit potent anabolic effects in the castrated LGD-3303- treated rats, all while lacking any discernible negative impacts to the prostate. Even at a dose as high as 300 mg/kg/day, the weight of the prostate in the LGD-3303-treated rats was equal to that of the control group (non-castrated, non-treated rats). Furthermore, LGD-3303 did not bring prostate weight to any more than 50% of that of the castrated rats, which is a very good indicator of its selectivity of muscle tissue over prostate tissue.
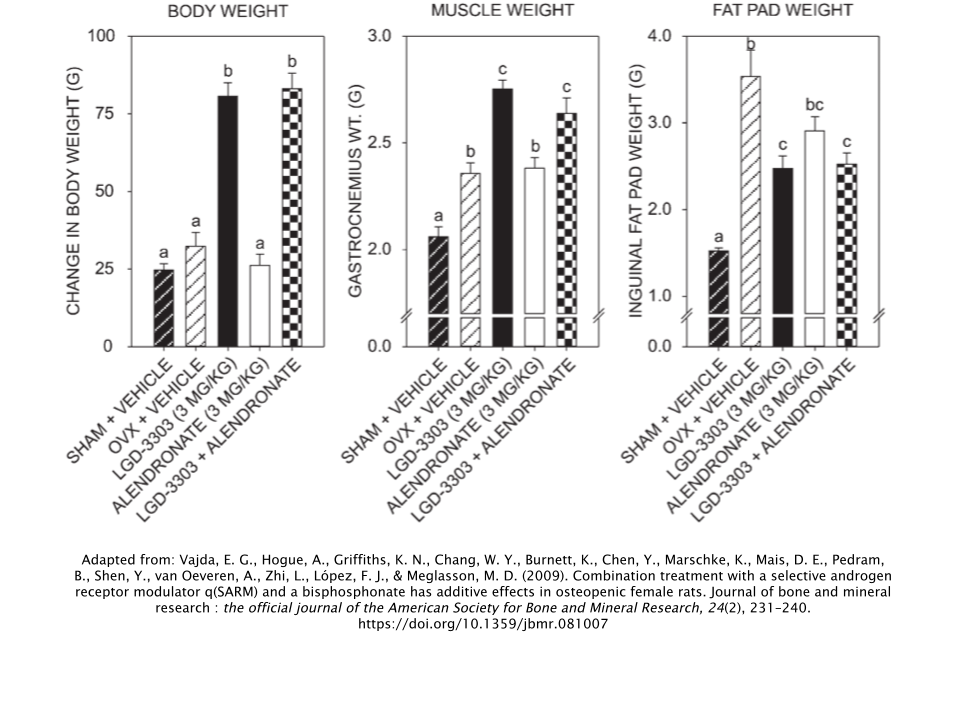
LGD-3303 was also able to increase the weight of female rats whose ovaries had been removed (oophorectomized), which is the equivalent of castration in males. At the same time, treatment with both LGD-3303 in isolation as well as in conjunction with the reference drug Alendronate (a drug used to treat osteoporosis) was able to significantly decrease fat storage, as measured by the weights of the rats’ inguinal fat pads [1].
Increased Bone Density
Since LGD-3303 was originally developed for individuals suffering from osteoporosis, we must also take a look at its effects on bone mineral content (BMC) and bone mineral density (BMD), the two primary measurements used in bone health studies.
The researchers who investigated LGD-3303’s effects on muscle and prostate also took a look at its effects on bone tissue in a separate group of female rats. What they found was that LGD-3303 was able to increase both the BMD and BMC of the lumbar spine (lower back) and the femur (thigh bone) in female rats that had been oophorectomized. This was shown both in isolation and with the aforementioned reference drug used for osteoporosis, Alendronate [1] 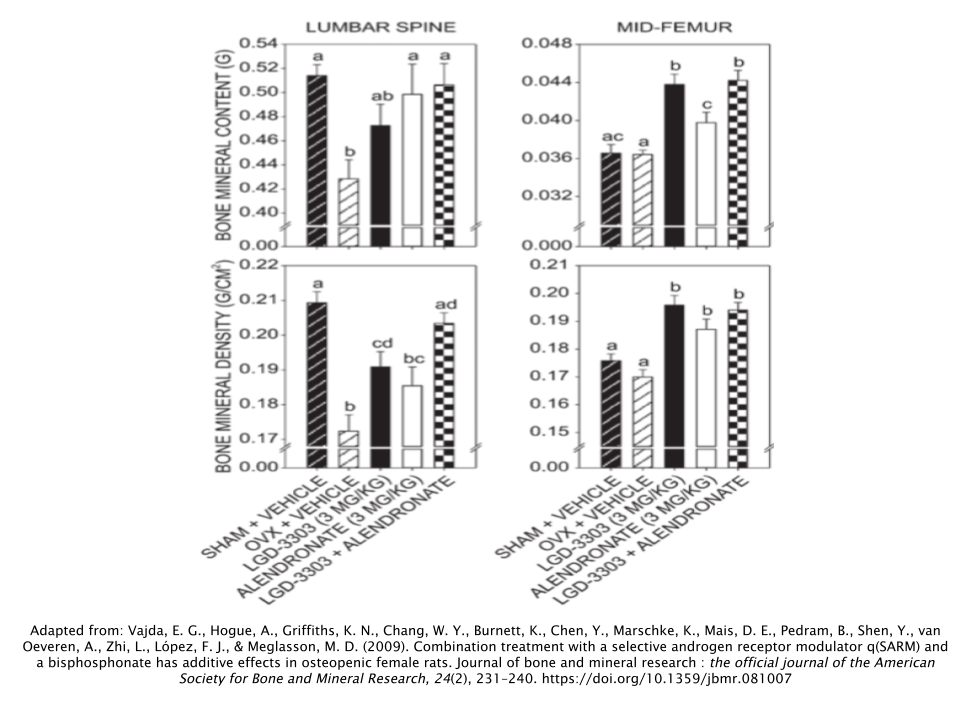
Why LGD-3303 is able to have these beneficial outcomes on bone tissue is that it’s able to reduce bone resorption and bone remodeling, both of which led to improved BMC, BMD, and biomechanical characteristics of the rats’ lumbar spine.
The reference drug Alendronate doesn’t exert this kind of anabolic activity in either bone or muscle, nor is there any approved therapy that has this combination of anabolic and anti-resorptive properties to date. This makes LGD-3303 an extremely valuable candidate for osteoporosis treatment, as it has demonstrated its ability to decrease bone fractures via two distinct mechanisms; increased bone strength and reduction of the incidence of falls.
Sexual Behavior
Interestingly enough, researchers aimed to examine LGD-3303’s role in sexual behavior. More specifically, how it could potentially resolve sexual desire disorders in women undergoing menopause.
The only option that women suffering from this type of libido disorder are to take androgens. However, this of course unfortunately comes with the increased risk of virilizing, or masculinization symptoms such as the enlargement of the clitoris, deepening of the voice, and increased amounts of body hair growth. Therefore, the potential for LGD-3303 to succeed in this area of clinical treatment would provide notable relief for these women who don’t have any other effective treatment options to turn to.
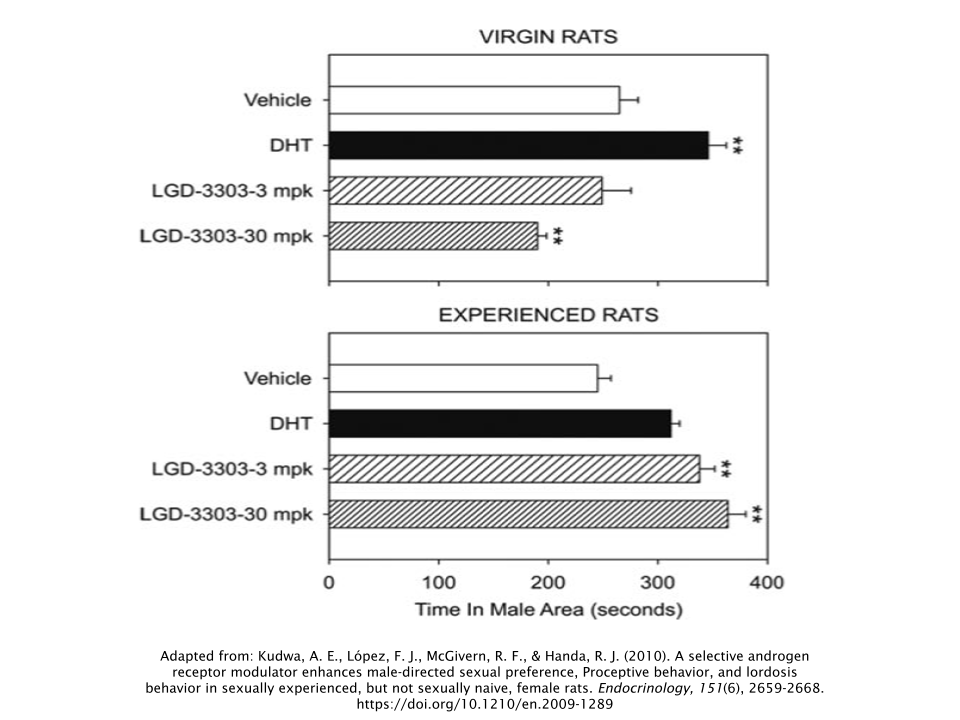
LGD-3303 has been shown to successfully enhance the behaviors associated with sexual desire in female rats towards male rats [3]. However, this effect was only observed in sexually-experienced (non-virgin) rats, as the virgin rats actually experienced a slight decrease in these same sexual behaviors. The researchers observed this phenomenon by how much time the female rats had spent on the male side of the “arena” during a sexual preference test.
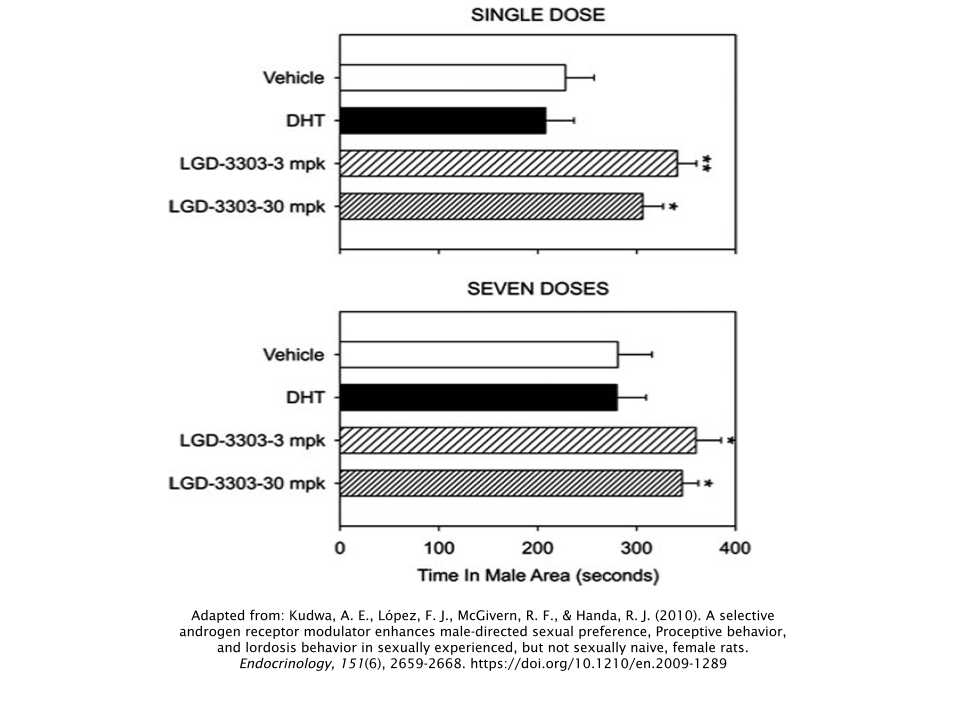
Increases in the sexual desires and preferences in sexually-experienced female rats occurred only after a single dose of LGD-3303 and increased only slightly after seven doses in both dosage groups (3 milligrams/kilogram and 30 milligrams/kilogram).
Side Effects
Since there is limited animal data and no clinical human data in which to draw any information from, it’s difficult to say what side effects (if any) are associated with the administration of LGD-3303. Since the animal data looks relatively “clean” in terms of side effects, it’s most likely safe to assume that LGD-3303 has a mild adverse effect profile.
But to err on the safe side, treat LGD-3303 as if it has the same side effect profile of other SARMs. This may include the lowering of “good” cholesterol (HDL) and the suppression of natural testosterone production.
Is LGD-3303 Better for Bulking or Cutting?
LGD-3303 appears to be very similar to LGD-4033 (Ligandrol), which is widely known as a bulking compound in anecdotal reports. The results observed in animal models appear to support this with its dramatic anabolic effects relative to its lack of androgenic effects. So it can be safe to assume that LGD-3303 would produce similar, if not identical, favorable outcomes in measures such as body composition and strength for a bulking cycle.
However, this isn’t to say that LGD-3303 wouldn’t be effective during other circumstances. It could be assumed that LGD-3303 would be able to help retain muscle tissue while undergoing a caloric deficit during a cutting phase and perhaps help to gain muscle during a body recomposition phase.
Dosages
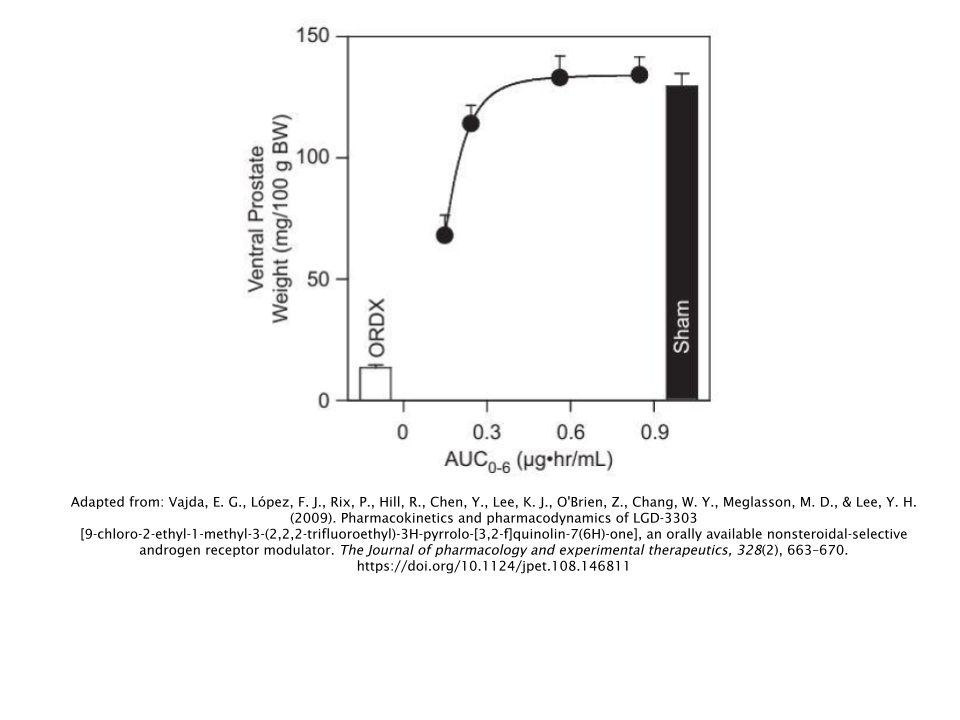
LGD-3303 looks as though it has a half-life of approximately 6-8 hours [2].
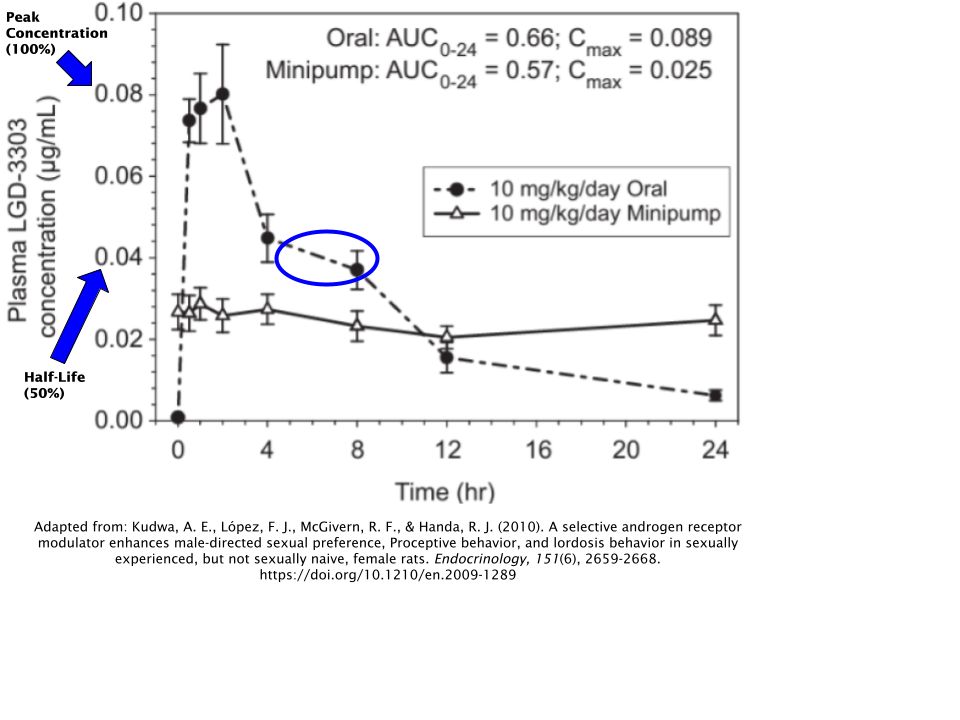
In the image above, you can see that the maximum (peak) concentration occurs at 0.08µg/mL and reaches its halfway point at 0.04µg/mL at approximately the 6-8 hour mark; illustrated by the blue oval.
This is a relatively short half-life compared to some other SARMs. So it’s important that if you are to take LGD-3303, you should dose it at least 2x/day. It might even be worth considering 3x/day dosing in order to maintain consistent blood levels over a 24-hour period.
How Does LGD-3303 Compare to Other SARMs?
As previously discussed, LGD-3303 is very similar on a physiological level compared to LGD-4033 (Ligandrol). 
They both seem like they’re able to produce similar results for muscle and strength gains. If any sort of speculation can be made regarding their differences, it’s that LGD-3303 may be a bit more effective for cutting and recomposition cycles than LGD-4033. This is because LGD-3303 appears to have slightly less androgenic effects than LGD-4033 does, provided the current data we have.
But take this with a grain of salt, as this may also be due to the fact that there is not nearly as much data on LGD-3303 as there is on LGD-4033.
Should I Use a Post-Cycle Therapy (PCT) After My LGD-3303 Cycle?
It’s recommended that those who’ve cycled with LGD-3303 should complete a PCT after they discontinue use. It’s safe to assume that this SARM suppresses testosterone just like any other SARM would. So the risks of suffering from a low testosterone condition increase drastically if one does not undergo a PCT after discontinuation of use. It’s better to err on the safe side here.
It’s not necessary to include aromatase inhibitors in your PCT. Using a selective estrogen receptor modulator (SERM) should suffice; the two most popular choices being either tamoxifen (Nolvadex®) or clomiphene (Clomid®). While using tamoxifen (Nolvadex®) is recommended due to its milder nature, some prefer the use of clomiphene (Clomid®). Either way, one or the other should be just fine. Rarely is it necessary to take both of these SERMs simultaneously in order to recover from a cycle of LGD-3303.
No matter which one you choose, here’s what a simple 4-week PCT protocol would look like for these SERMS:
| Week | Tamoxifen (Nolvadex®) | OR | Clomiphene (Clomid®) |
|---|---|---|---|
| 1 | 40 mg/day | 50 mg/day | |
| 2 | 40 mg/day | 50 mg/day | |
| 3 | 20 mg/day | 25 mg/day | |
| 4 | 20 mg/day | 25 mg/day |
References
- Vajda, E. G., Hogue, A., Griffiths, K. N., Chang, W. Y., Burnett, K., Chen, Y., Marschke, K., Mais, D. E., Pedram, B., Shen, Y., van Oeveren, A., Zhi, L., López, F. J., & Meglasson, M. D. (2009). Combination treatment with a selective androgen receptor modulator q(SARM) and a bisphosphonate has additive effects in osteopenic female rats. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research, 24(2), 231–240. https://doi.org/10.1359/jbmr.081007
- Vajda, E. G., López, F. J., Rix, P., Hill, R., Chen, Y., Lee, K. J., O’Brien, Z., Chang, W. Y., Meglasson, M. D., & Lee, Y. H. (2009). Pharmacokinetics and pharmacodynamics of LGD-3303 [9-chloro-2-ethyl-1-methyl-3-(2,2,2-trifluoroethyl)-3H-pyrrolo-[3,2-f]quinolin-7(6H)-one], an orally available nonsteroidal-selective androgen receptor modulator. The Journal of pharmacology and experimental therapeutics, 328(2), 663–670. https://doi.org/10.1124/jpet.108.146811
- Kudwa, A. E., López, F. J., McGivern, R. F., & Handa, R. J. (2010). A selective androgen receptor modulator enhances male-directed sexual preference, Proceptive behavior, and lordosis behavior in sexually experienced, but not sexually naive, female rats. Endocrinology, 151(6), 2659-2668. https://doi.org/10.1210/en.2009-1289