
LGD-4033: The Complete Guide
*DISCLAIMER: Selective Androgen Receptor Modulators (SARMs) are not approved by the FDA for any currently acceptable medicinal/therapeutic purpose. Therefore, this article does not serve as medical advice and is not to be intended to be used to diagnose, treat, cure or prevent any disease. SARMS are to be used for research purposes only and not intended for human consumption.*
What is LGD-4033?
LGD-4033, better known in the fitness and bodybuilding communities as Ligandrol, is a type of nonsteroidal selective androgen receptor modulator (SARM). Currently it is being investigated as a treatment for muscle-wasting conditions, such as multiple sclerosis and certain types of cancers [1].
As of the publication of this writing, it is in development by Viking Therapeutics, who purchased the rights to investigate the drug from Ligand Pharmaceuticals back in 2014. Viking is investigating the drug (unofficially changing the name of LGD-4033 to VK5211 in the process) for its potential in the treatment of cancer cachexia; a type of muscle-wasting cancer commonly associated with symptoms such as anemia and significant weight loss. According to the company, the drug should hypothetically bring about similar benefits experienced by those who’ve undergone testosterone treatment, but with greater amounts of safety and tolerability. This has been hypothesized to stem from LGD-4033’s tissue-selective mechanism and oral route of administration, as opposed to the typical intramuscular injection route of anabolic steroid treatments such as testosterone [2].
How does it work?
In order to understand how LGD-4033 works, we must first look at its relationship with the androgen receptor (AR). The AR is primarily activated by androgenic hormones such as testosterone and dihydrotestosterone (DHT), certain peptides like insulin, and growth factors such as human growth hormone (HGH). This leads to a cascade of events; ultimately leading to both positive and negative effects. Positive effects include those of an anabolic nature, such as increases in muscle and strength [3]. On the other hand, the most prominent example of a negative effect is growth of the prostate, which may unfortunately lead to prostate cancer [4].
LGD-4033 is of great interest to both clinicians and recreational users alike due to its unique, selective nature. It possesses the ability to increase skeletal muscle accretion and bone density, while simultaneously inhibiting undesirable tissue growth (i.e. breast and prostate). Growth of the latter type is unfortunately common with traditional testosterone treatment and a common reason as to why this therapy is avoided in clinical settings [5].
There are a few aspects about LGD-4033 that make it quite unique;
Non-steroidal
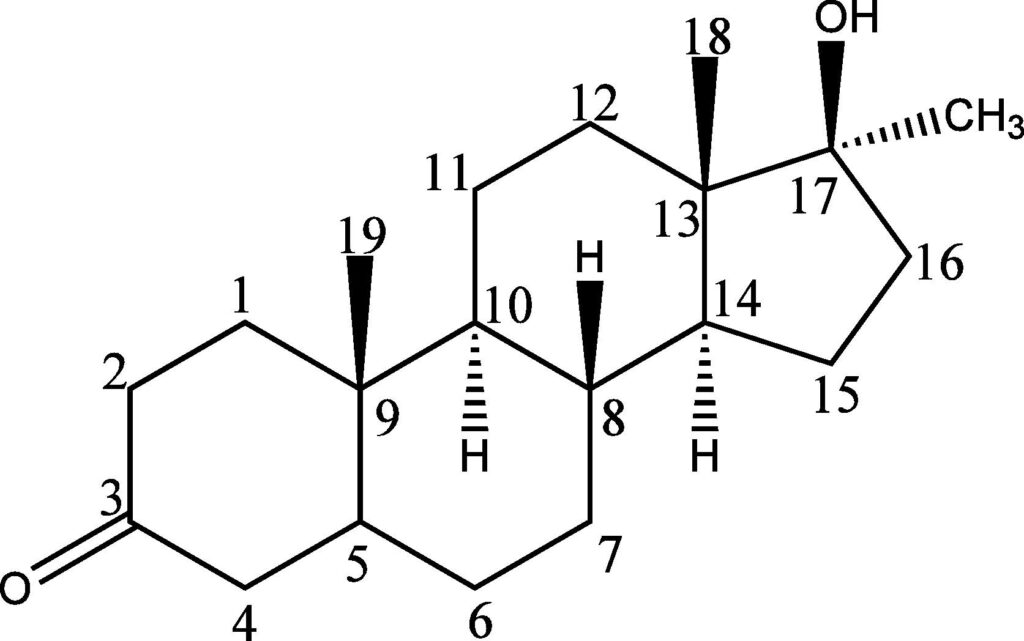
The drawback to taking testosterone (or any of its derivatives) is the potential, as well as the extent, to which aromatization or 5-α(alpha)-reduction occurs. This refers to the conversion of testosterone to estrogen or DHT, respectively [6]. Dependent upon the amount of testosterone that is administered, excess amounts of either hormone could potentially lead to deleterious effects. An excess of estrogen in circulation may result in increased fat storage and/or gynecomastia (“bitch tits”), while too much DHT can lead to detrimental effects on the prostate, such as the development of prostate cancer [4].
Since LGD-4033 is not a steroidal hormone like testosterone, it (hypothetically) should not lead to the aforementioned drawbacks associated with testosterone therapy/administration.
Orally Ingested
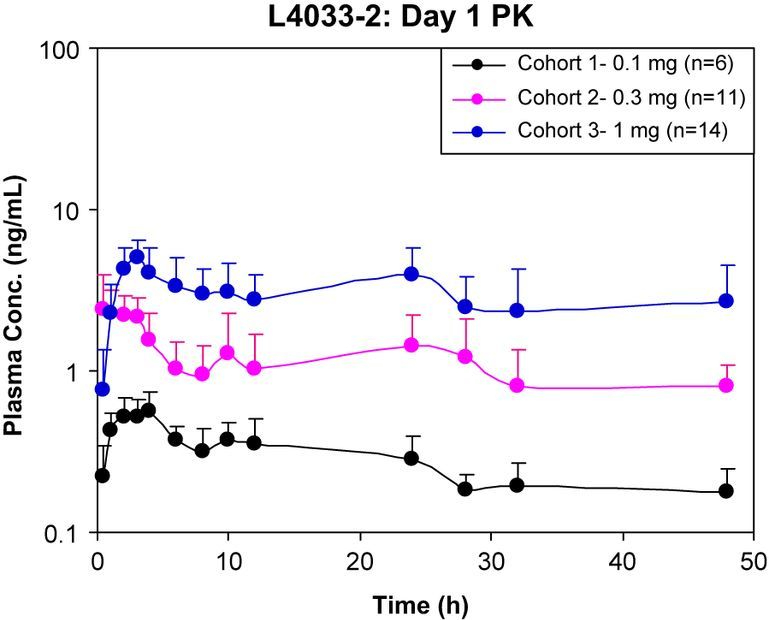
LGD-4033 has an elimination half-life of 24-36 hours. That’s quite a long period of time for an orally-ingested anabolic agent [7]. Because of its long half-life, an individual would not have to take the drug any more than 1x/day, and perhaps could get away with 1x/every other day, in theory. And of course, the drug does not have to be administered by injection, which is a turn-off to many people.
High AR Affinity
Affinity, in this context, means how “tightly” the SARM is binding to the AR. LGD-4033 and its high level of affinity to bind to the AR is the reason as to why it is so “selective” in its nature. Compared to testosterone, LGD-4033 is exponentially more selective [7]. This, in theory, prevents negative effects commonly associated with testosterone/anabolic steroid treatment, such as hypertrophy (growth) of the prostate or anabolic-steroid-induced hypogonadism (ASIH).
Animal Data
In order to study the endocrine, or hormonal, effects of a particular drug treatment, one method that researchers use is what is called an ovariectomized female rat model. What this means is that the female rats’ ovaries were removed, which could be equated to castration, or removal of the testicles, in males. This specific model is specifically used to replicate a population of postmenopausal women in humans.
A study utilizing this type of study design examined the effects of 3 doses of LGD-4033 over the course of 5 weeks. The lowest dose was calculated based on an amount that would hypothetically result in improvements in lean body mass (LBM). Due to a lack of human data on SARMS in general, this calculation was made based on a previous human trial with GTx-024, otherwise known as Ostarine or Enobosarm, which came out to 0.04 mg/kg/BW (meaning “milligrams per kilogram of body weight”) [8]. In order to investigate the possibility of a dose-dependent effect, the next 2 treatment groups used this previously calculated dose and had it multiplied by factors of 10x and 100x, resulting in 0.4 mg/kg/BW and 4 mg/kg/BW, respectively.
The main takeaways from this study are that higher doses (exceeding therapeutic levels, such as those using it for bodybuilding/recreational use) may lead to the drug having a weaker level of selectivity. This was illustrated in the study by the significant increase in the weight of the ovariectomized rats’ uterus.
Also, the amount of skeletal muscle vascularization was also shown to increase in the ovariectomized rats who took LGD-4033. Skeletal muscle vascularization has been hypothesized to be one of the key components of muscle regeneration [9]. Therefore, this data could potentially be extrapolated to humans and be used as a beneficial recovery compound after resistance training.
Human Data
There is one notable study from Boston Medical Center that has often been cited by various recreational users of LGD-4033 due to its high-quality study design, which is rare for a drug that is only in Phase II of clinical trials (with successful completion of Phase III trials being needed to proceed to an FDA-approval).
In this study, 68 healthy men with normal levels of testosterone were assigned to different groups. Each participant was instructed to take a different dose of LGD-4033; either 0 mg/day (placebo), 0.1 mg/day, 0.3 mg/day, or 1.0 mg/day, for 3 weeks [7].
Safety
LGD-4033 was shown to be very safe and well-tolerated amongst all study participants, with the only reported side effects being that of headache and a dry mouth. The participants’ LDL, or “bad cholesterol” was not significantly affected, but HDL, or “good cholesterol” had notably declined at the 0.3 and 1.0 mg/day dosages. Fortunately, HDL cholesterol levels had returned to normal after the subjects had stopped taking the LGD-4033. None of the subjects in any of the groups experienced changes in their liver enzymes, prostate specific antigen (PSA), or electrocardiogram (ECG):
Liver Enzymes
These enzymes are often negatively impacted by the ingestion of oral anabolic steroids, such as methandienone, or Dianabol. These types of steroids must undergo a chemical change called 17-α(alpha)-alkylation in order to successfully bypass the liver. This, in turn, can cause liver damage, or hepatotoxicity [10] [11].
Prostate-specific antigen (PSA)
This is a biomarker often included in blood panels as a method of detecting the risk of developing prostate cancer [12].
Electrocardiogram (ECG)
This is a test that measures the activity of the heart and can detect cardiac pathologies such as left ventricular hypertrophy (LVH); an increase in muscle thickness of the heart’s left ventricle, which is responsible for pumping oxygenated blood to the rest of the body. LVH is often experienced by anabolic-androgenic steroid users [13].
The lack of change in the variables listed above illustrates that, at least relative to exogenous testosterone/anabolic steroid administration, LGD-4033 possesses a much more impressive safety profile compared to its anabolic steroid counterparts.
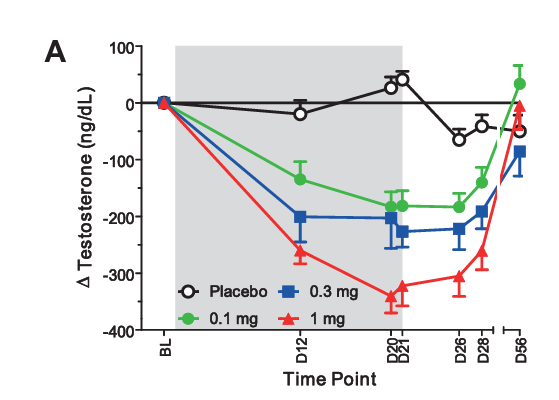
Testosterone Suppression
The subjects in the study experienced a dose-dependent suppression of total testosterone. In other words, this means that greater levels of testosterone suppression were seen at higher doses of LGD-4033, and vice-versa. Sex-hormone binding globulin (SHBG), a hormone that binds to testosterone and prevents it from exerting its actions on the body, was suppressed in a dose-dependent manner similar to total testosterone.
The researchers also examined the subjects’ free testosterone. This represents the amount of testosterone not bound by SHBG, which makes up anywhere from about 0.5% – 3% of total testosterone in the average male [14]. Free testosterone was only suppressed in the highest dosage group of 1.0 mg/day. This is surprising, given the fact that SHBG was suppressed in a dose-dependent fashion. One could hypothesize that free testosterone should have increased in a dose-dependent fashion as well, provided the fact that SHBG and free testosterone share an inverse relationship with one another. Simply put, if there is less SHBG available to bind to testosterone, there should theoretically be greater amounts of free testosterone in circulation. Unfortunately, however, this was never addressed by the researchers.
It should be noted that after the participants had stopped using the SARM after 3 weeks of treatment, their hormone levels had returned to normal.
Body Composition & Performance Parameters
There was also a dose-dependent increase in LBM, with the 1.0 mg/day group seeing an average of a 1.21 kg (2.67 lbs) increase over the course of the 3 week study period. Fat mass had not changed to any notable degree in any of the groups.
While the researchers had included a stair-climbing test in order to assess speed and power, the treatment groups’ extremely modest performance improvement did not reach statistical significance (which can be viewed as the extent of improvement needed in order for the result to be considered as scientifically valid).
Is LGD-4033 Better for Bulking or Cutting?
LGD-4033 is better known as a bulking SARM due to its very high amounts of anabolic activity. There are some users that have anecdotally reported over a cycle of 1-2 months, they gained 5-10 lbs of LBM. This is quite impressive relative to other SARMs. But it’s important to note that individual results will vary drastically from one person to the next, as anecdotal reports do not have any sort of control standards, and should be taken with a grain of salt. And the obvious must be stated here; make sure you’re in a calorie surplus if you’re looking to build muscle!
While there are some anecdotal reports that mention water retention while using LGD-4033, this most likely has to do more with the person’s diet and exercise regimen rather than the SARM itself. This can be assumed from the fact that LGD-4033 does not convert to estrogen (which is notorious for causing individuals to hold water when taking high amounts of testosterone), therefore, any sort of edema is not likely to occur.
How Does LGD-4033 Compare to Other SARMS?
GTx-024 (Ostarine) (Enobosarm)
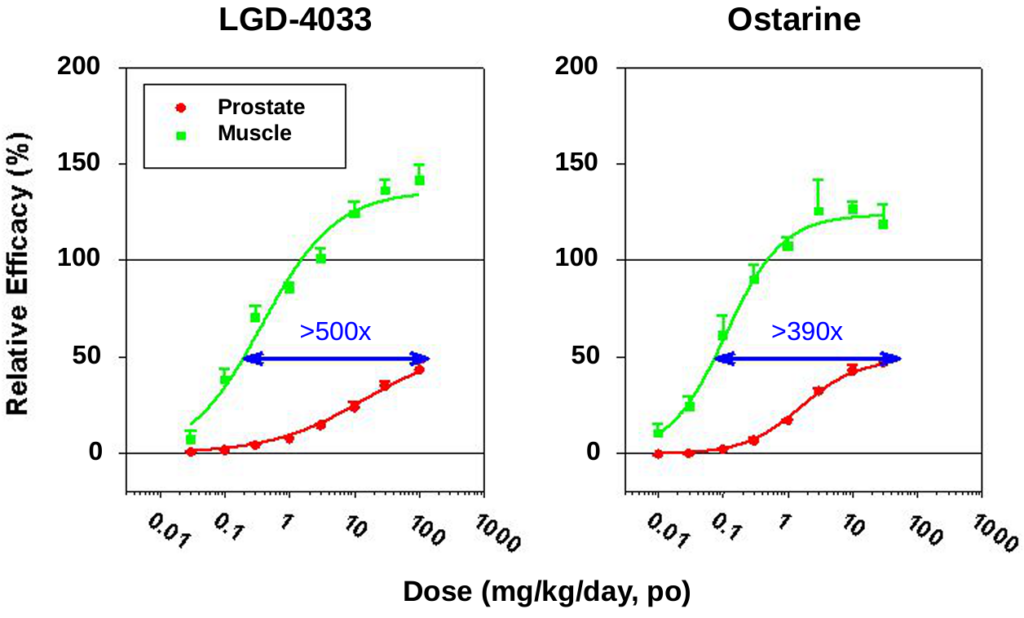
In a male rat model for hypogonadism, LGD-4033 was shown to have significantly greater selectivity for the androgen receptor compared to Ostarine; with LGD-4033 having 500x the selectivity of testosterone and Ostarine having only 390x the selectivity of testosterone [15]. This is illustrated by administration of LGD-4033 resulting in greater rates of muscle accretion, with similar effects on the prostate.
RAD140 (Testolone)
Testolone still does not have any human clinical data to back it up, so it’s tough to compare these 2 SARMs together. However, anecdotal evidence tells us that testolone is a bulking compound just like LGD-4033. So theoretically any one of these would make a good choice for bulking. Some seem to have better luck with one compared to the other, for reasons we can’t even begin to postulate at this point due to the lack of available human data.
S23
As with testolone, S23 is still in its preclinical stages with no human data available to establish its potential to contribute to significant LBM gains in humans. What’s interesting about S23 is that it is actually being investigated as a male hormonal contraceptive; having the highest level of binding affinity to the AR compared to any other SARM to date.
This means that S23 is extremely suppressive to testosterone levels. It’s so suppressive that administration of 0.1mg/day of S23 to rats for only 14 days caused a > 50% decrease in luteinizing hormone (LH); a hormone responsible for stimulating the Leydig cells of the testicles, leading to the synthesis of testosterone [16]. So experimenting with this SARM has a much less friendly safety profile compared to LGD-4033.
However, in this same study S23 was shown to increase bone mineral density and LBM, while also reducing fat mass in a dose-dependent manner.
Anecdotal reports are supportive of its muscle-building/fat-loss potential, making it suitable for both bulking and cutting. But if you want to err on the more conservative side, it might be best to stick with LGD-4033. This is especially true if you’re committed to a bulking cycle.
Recreational Dosage Amounts
Based upon data gathered from the only human study that is available to us as of the publication of this article, we could presumably expect a modest increase in LBM of ~2.5 lbs. This, of course, assumes that the individual uses the 1.0 mg/day dosage; the highest-dosed group in that particular study [7].
Similar to what’s traditionally seen with recreational anabolic steroid users, there are individuals that are going to take dosage amounts of LGD-4033 that exceed the established therapeutic amount. So caution must be exercised. But with this SARM, however, the room for error appears to be quite large. This is due to the fact that a single-ascending dose Phase I trial of LGD-4033 in rats demonstrated that up to 22 mg/day was well-tolerated with no adverse effects reported [15].
While there’s obviously no established dose of LGD-4033 for those simply looking to build more muscle and enhance their physique, there are many anecdotal reports out there. Combining this from what we can extrapolate from the data that we do have at our disposal, we can provide decently reasonable estimates for appropriate dosage amounts.
The goal here is make sure we hit what’s called the minimum effective dosage (MED). This ensures that an individual is able to reach their muscle-building goals, while at the same time, not putting themselves at an unnecessary level of risk such as increasing the amount of time one’s testosterone is suppressed. The MED will vary from person to person, and will take some guess-and-check work at the end of the day.
With all this in mind, a general guideline to help you get started would look something like this:
- Men: 10-20 mg/day for 8 weeks
- Women: 5-10 mg/day for 8 weeks
Remember, keep the MED in mind and always start at the lower end of the range. If you find that LGD-4033 appears to be well-tolerated for you after a few days, titrate up the dose amount (~1mg every few days or so) if you don’t begin to see any results. On the opposite end of the spectrum, make sure to lower your current dose amount (or even discontinue use completely) if you’re experiencing side effects.
Potential Side Effects
Many of the side effects we’ve discussed thus far are things you can’t necessarily “feel”, such as lowering of your good cholesterol and testosterone suppression. So are there any side effects that you should be aware of that may occur during your cycle?
While it must be stated that results from person to person are always going to differ, it needs to be stated. Also, the data that is currently available to us only uses therapeutic dosage amounts in humans. So taking the aforementioned recreational dosage amounts commonly seen in anecdotal reports may result in side effects not seen in the study we discussed earlier.
Androgenic Side Effects
Given what is known about LGD-4033 and its mechanism of action, it still exerts actions upon the androgen receptors of the body. While this SARM is much more selective than testosterone in regards to the tissues it exerts androgenic activity upon, it still increases systemic (overall) levels of androgenicity within the body. So there is still a possibility for androgenic side effects to occur, such as hair loss, acne, and oily skin.
Estrogenic Side Effects
Since LGD-4033 does not aromatize into estrogen, it may be possible that a low estrogen condition develops while taking high amounts of the SARM for an extended period of time. As we know, LGD-4033 suppresses testosterone in a dose-dependent manner. So theoretically, with less testosterone present, there is less estrogen to be aromatized. While lower estrogen inherently sounds like a good thing, this is not actually the case. Low levels of estrogen could potentially result in symptoms such as decreased strength, appetite, and libido, as well as overall fatigue and lethargy.
This is all just theoretical, of course. Although there is no data currently to support this claim, it’s still something important to keep in mind when using LGD-4033.
Testosterone Suppression
The human study reported that suppression of total testosterone occurred in a dose-dependent manner. While free testosterone was negatively impacted only in the 1.0 mg/day group, it’s important to remember that recreational doses of this SARM are 10-20x this amount. Therefore, it can be postulated that this negative effect on free testosterone would be amplified in a dose-dependent manner, similar to levels of total testosterone.
The lowering of free testosterone to a significant extent may result in symptoms such as:
- Low lipido
- Increased rate of fat gain
- Decreased muscle size and strength
- Depression
- General fatigue
Should I Use a Post-Cycle Therapy (PCT) After My LGD-4033 Cycle?
Yes. Those who’ve cycled with LGD-4033 should absolutely complete a PCT after they discontinue their use of LGD-4033. Since this SARM has been shown to suppress testosterone, risks of suffering from a low testosterone condition increase drastically if one does not undergo a PCT after discontinuation of use.
Since this SARM has a half-life of 24-36 hours, one should start their PCT the day after they stop taking LGD-4033.
It’s not necessary to include aromatase inhibitors in your PCT. Using a selective estrogen receptor modulator (SERM) should suffice; the two most popular choices being either tamoxifen (Nolvadex®) or clomiphene (Clomid®). While using tamoxifen (Nolvadex®) is recommended due to its milder nature, some prefer the use of clomiphene (Clomid®). Either way, one or the other should be just fine. Rarely is it necessary to take both of these SERMs simultaneously in order to recover from a cycle of LGD-4033.
No matter which one you choose, here’s what a simple 4-week PCT protocol would look like for these SERMS:
| Week | Tamoxifen (Nolvadex®) | OR | Clomiphene (Clomid®) |
| 1 | 40 mg/day | 50 mg/day | |
| 2 | 40 mg/day | 50 mg/day | |
| 3 | 20 mg/day | 25 mg/day | |
| 4 | 20 mg/day | 25 mg/day |
References
- National Center for Biotechnology Information (2021). PubChem Compound Summary for CID 44137686. Retrieved July 11, 2021 from https://pubchem.ncbi.nlm.nih.gov/compound/lgd-4033.
- Viking signs broad licensing deal with ligand pharmaceuticals for rights to five novel therapeutic programs. (2014, May 22). Viking Therapeutics. Retrieved July 11, 2021, from https://www.vikingtherapeutics.com/2014/05/22/viking-signs-broad-licensing-deal-with-ligand-pharmaceuticals-for-rights-to-five-novel-therapeutic-programs/
- Bhasin, S., Storer, T. W., Berman, N., Callegari, C., Clevenger, B., Phillips, J., Bunnell, T. J., Tricker, R., Shirazi, A., & Casaburi, R. (1996). The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. The New England journal of medicine, 335(1), 1–7. https://doi.org/10.1056/NEJM199607043350101
- Fujita, K., & Nonomura, N. (2019). Role of Androgen Receptor in Prostate Cancer: A Review. The world journal of men’s health, 37(3), 288–295. https://doi.org/10.5534/wjmh.180040
- Fragkaki, A. G., Sakellariou, P., Kiousi, P., Kioukia‐Fougia, N., Tsivou, M., Petrou, M., & Angelis, Y. (2019). Human in vivo metabolism study of LGD‐4033. Drug Testing and Analysis, 12(1), 164-164. https://doi.org/10.1002/dta.2700
- Gao, W., & Dalton, J. T. (2007). Ockham’s razor and selective androgen receptor modulators (SARMs): are we overlooking the role of 5alpha-reductase?. Molecular interventions, 7(1), 10–13. https://doi.org/10.1124/mi.7.1.3
- Basaria, S., Collins, L., Dillon, E. L., Orwoll, K., Storer, T. W., Miciek, R., Ulloor, J., Zhang, A., Eder, R., Zientek, H., Gordon, G., Kazmi, S., Sheffield-Moore, M., & Bhasin, S. (2013). The safety, pharmacokinetics, and effects of LGD-4033, a novel nonsteroidal oral, selective androgen receptor modulator, in healthy young men. The journals of gerontology. Series A, Biological sciences and medical sciences, 68(1), 87–95. https://doi.org/10.1093/gerona/gls078
- Dalton, J. T., Barnette, K. G., Bohl, C. E., Hancock, M. L., Rodriguez, D., Dodson, S. T., Morton, R. A., & Steiner, M. S. (2011). The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: results of a double-blind, placebo-controlled phase II trial. Journal of cachexia, sarcopenia and muscle, 2(3), 153–161. https://doi.org/10.1007/s13539-011-0034-6
- Kamal Ranjbar and Bayan Fayazi (May 2nd 2019). Vascularisation of Skeletal Muscle, Muscle Cells – Recent Advances and Future Perspectives, Mani T. Valarmathi, IntechOpen, DOI: 10.5772/intechopen.85903.
- Girgis, C. M., Kuo, I., & Handelsman,, D. J. (2014). Acute hepatitis and fevers in an amateur body-builder: A new complication of synthetic androgen abuse? Endocrine Practice, 20(8), e130-e133. https://doi.org/10.4158/ep14034.cr
- Bond, P., Llewellyn, W., & Van Mol, P. (2016). Anabolic androgenic steroid-induced hepatotoxicity. Medical hypotheses, 93, 150–153. https://doi.org/10.1016/j.mehy.2016.06.004
- Velonas, V. M., Woo, H. H., dos Remedios, C. G., & Assinder, S. J. (2013). Current status of biomarkers for prostate cancer. International journal of molecular sciences, 14(6), 11034–11060. https://doi.org/10.3390/ijms140611034
- Urhausen, A., Albers, T., & Kindermann, W. (2004). Are the cardiac effects of anabolic steroid abuse in strength athletes reversible?. Heart (British Cardiac Society), 90(5), 496–501. https://doi.org/10.1136/hrt.2003.015719
- Belchetz, P. E., Barth, J. H., & Kaufman, J. M. (2010). Biochemical endocrinology of the hypogonadal male. Annals of clinical biochemistry, 47(Pt 6), 503–515. https://doi.org/10.1258/acb.2010.010150
- Higgins, John. June 24, 2010. Investor and Analyst Day, Exhibit 99.1. Ligand Pharmaceuticals, Inc. https://www.sec.gov/Archives/edgar/data/886163/000119312510146054/dex991.htm
- Jones, A., Chen, J., Hwang, D. J., Miller, D. D., & Dalton, J. T. (2009). Preclinical characterization of a (S)-N-(4-cyano-3-trifluoromethyl-phenyl)-3-(3-fluoro, 4-chlorophenoxy)-2-hydroxy-2-methyl-propanamide: a selective androgen receptor modulator for hormonal male contraception. Endocrinology, 150(1), 385–395. https://doi.org/10.1210/en.2008-0674